This video shows a macular hole which looks like a small orange area in the centre of the green just below the tiny tweezers! The retina has been stained with ICG (although I rarely use this it does show the peeling of the surface of the retina well!) I mainly use a blue dye which you may see me put into the eye.
You will see me grab the surface layer called the ILM (Internal Limiting membrane) and then peel it around in a circle. You may see this in surgery but patients often describe it as happening in the distance like a Chinese theatre. It is not scary at all and I had one patient disappointed because she saw the peel on the first eye but did not see it on the second as sometimes the anaesthetic dulls the vision!
You have seen the peel bit above. This is the entire procedure sped up 8x and I am grateful to the patient for giving me permission to share it. He is also a surgeon and I hope will enjoy it! I start by putting the ports into the eye whilst it is firm. Then it is time to remove the cataract and place a lens into the bag. I prefer to include cataract surgery as it speeds up recovery and saves the Patient (And the NHS!) another day of surgery and the multiple out patient visits that result! Once the cataract is out I take the back of the capsule away saving a YAG laser procedure at a later day (Yet another trip to the hospital for the patient). Next I lift the gel off the back of the eye (Inducing a PVD) and then perform a once round the eye, smooth movement vitrectomy. The gel is cut at 5000x per minute and then sucked away. It is during the induction of a PVD and the vitrectomy that tears may form on the retina. With the gel gone a blue stain is put onto the retina and then the ILM is peeled. After a search for any tears the eye is filled with air and then the air is changed for gas. I use the shortest acting gas I can. For small holes it is SF6 which lasts for two weeks and for very large holes I will use C3F8 which lasts for two months. I will usually use oil in previous failures. It is very comfortable surgery, there is nothing to worry about!
Macular Hole CLICK HERE FOR PATIENT INFORMATION LEAFLET
What is a macular hole?
A macular hole is a hole that develops in the macula! The macula is the central part of the retina (the light sensitive film in the camera that is the eye) and right at the centre of the centre is a dip called the fovea. This is the only place we can see detail. (Just try looking at a clock right now, then look about 1m to the side and try to read the clock, you cannot!) So when a hole forms at this part of the retina, the ability to see detail goes, the world becomes blurred and often there is distortion which classically squashes faces into the centre.
Why has this happened?
The Jelly of the eye separates right at the back first of all. In some people (mainly women in their late 60s, the Jelly holds onto the centre and pulls a bit of retina out causing a hole. Fluid then starts to build up around the edge. Most of the time the cause is idiopathic (which means we do not know!), sometimes it can be caused by trauma and sometimes by scar tissue on the surface pulling the retina hard.
What can be done?
Until the early 1990s nothing but now, we have very successful techniques to close these holes over 90% of the time. Surgery involves removing forces that hold the hole open and allowing the eye to heal itself. Surgery is done under a local anaesthetic and is completely comfortable. If you wanted to have some 'chemical courage', sedation can be given to relax you.
I will routinely take the lens (cataract) as there is usually early cataract. I get a better view to do surgery with the cataract out, I can get more gas into the eye and the patient is saved a second operation as Vitrectomy (Removing the Jelly) causes cataract. Once the cataract is out the jelly is removed (Vitrectomy) by a tiny guillotine which cuts the jelly into tiny pieces 5000 times a minute and then sucks it away. A salt water drip keeps the eye inflated during this removal. With the jelly out the surface layer of the eye is peeled just enough to remove any pulling forces acting as a draw bridge to lift the edges of the hole. Finally a gas bubble is put in to seal off the hole and allow the retina to pump flat again. I do not posture but some surgeons do and that is fine! The gas bubble stays in for 2 weeks up to 2 months depending on the gas used (some absorb into the blood more quickly than others). You cannot see with gas in the eye and as it goes you begin to feel like a human spirit level with a fluid level bouncing around. The shadow from the gas gets smaller, rounder and lower with time until it suddenly goes. You cannot fly with gas in the eye or go up mountains as the gas would expand and the pressure become very high in the eye and that hurts. If the hole is big I use the long acting gas, if it is small the short acting gas, I want you to get back to normal as quickly possible.
Should I have it done?
Nobody jumps out of a second floor window, If a Lion walked into the room most would jump! If you choose not to have surgery the vision is very likely to get worse until only the top letter of the test chart can be seen. Doing nothing usually results in very poor vision although small holes can sometimes close on their own. So if you want to see better then surgery is the only option (Although injection treatments might work on small holes) The main risk that I would consider significant as a patient is the risk of retinal detachment at around 3%. A careful check is made at the end of the operation and any holes in the retina at the edge that can result in retinal detachment are treated. Vision usually improves several lines down the chart on average but vision continues to improve over years.
A patient Story- Mrs M
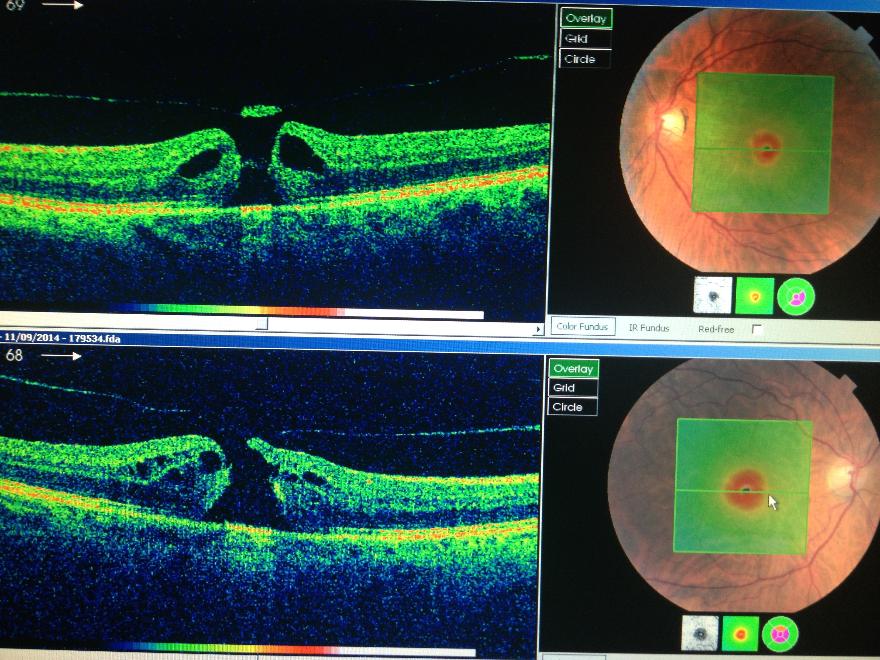
Mrs M (Thanks for letting me share!) presented with blurred vision and was seen by her optometrist who made the diagnosis and referred her. I saw her on 19th September. Vision was very poor and well below the standard for driving at Right 0.74, Left 0.72. This around 6/36 or about three lines down from the big letter at the top of the test chart you read when you get your eyes tested. Her OCT scans are shown below.
The top picture is of the left eye and on the right side of this picture there is a small picture of the retina as if the eye is looking straight at you. (This is the red eye of photography in focus!). The white area on the left is the optic nerve and this is 1.5mm in size. The big dark blood vessels are veins and the lighter smaller ones are arteries. This picture has a green box overlaying the middle part of the retina, the macula. Think of this like a geography map showing you a landscape where green is the colour of ground level (like grass), yellow shows a normal amount of thickening of the ground but red shows hills which should not be there and white would represent snow on top of mountains. The normal retina would show up as a green field with a blue puddle in the middle because at the very centre of the macula is a dip called the fovea, which is the only part of the eye we can all see detail with. Because it is a dip it is thinner, hence in these maps it should be coloured blue. Through the centre of this picture is a green line which is the line we will cut through to put the retina facing up.
The left picture shows a cross section through the retina at the level of the green line. The patient is effectively on their back looking straight up. Starting at the bottom of the picture you can see a dark area and then speckled green. This is the white of the eye and the blood vessel layer under the retina called the choroid. The red line is the layer on which the retina sits. The ten layers of the retina can be seen above this red line and you can immediately see that there is a gap in the middle with a blister of fluid either side (dark areas) and in the middle of the gap is a bit of retina stuck to the jelly which can be seen as a very fine line going from left to right. The Jelly has pulled this little plug out and this has caused the little hole. The gap is tiny at around one quarter of a mm!
The bottom picture is the right eye and here you can see that the plug has not yet been fully pulled free but there is still a gap. This hole is a little younger than the top picture.
Mrs M was unusual in that she came along with a hole in both eyes at the same time. We discussed surgery and she was keen and so we got on with the surgery very quickly with the right operated on 25 the September and the left on the 9 October. Surgery was uncomplicated and she had both lenses replaced, the retinas peeled and gas in each eye. The first eye had a 'five week gas' and the second a 'two week gas' and there was no need to posture! I saw her again after surgery on 24 Octoberand rescanned her eyes. The Post operative OCT scans are shown below. (Forgive the quality they are actual photos of the screens!)
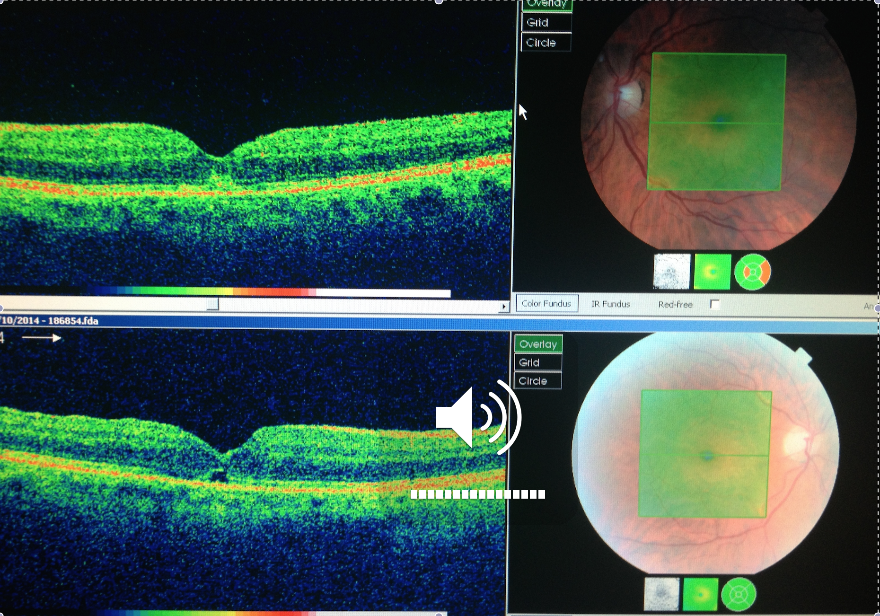
She had been very comfortable after surgery and vision was now 0.30 in the right and 0.20 in the left. This is around 6/12 in the right eye and 6/9 in the left or just over over half way down the test chart. With this level of vision she would be very close to passing the number plate test for driving as the equivalent line on the test chart for the number plate test is around 6/10. I saw her again on the 21 January 2015 and vision had improved another line in the right eye to 6/9 and the left was now seeing 6/6. 6/6 is better known as 20/20 vision. Vision seems to improve for several years following macular hole surgery. She was happy and so was I , a good outcome!

|
Personal Macular Hole Patient information leaflet.docx Size : 796.626 Kb Type : docx |